How RPE Works
Regenerative Periodontal Endoscopy: Before and after pictures and x-rays
How Regenerative Periodontal Endoscopy Works:
Regenerative Periodontal Endoscopy, or RPE, is an advanced non-invasive endoscope procedure pioneered and offered by PerioPeak Innovations. The skilled use of a periodontal endoscope (perioscopy), micro-ultrasonic piezo technology, and regenerative proteins can eliminate the need for aggressive surgery. When used properly, dental endoscope technology allows for pinpoint precision and the complete removal of tartar/calculus in deep pockets without the need for surgery. Emdogain, a natural regenerative protein, is then placed on properly prepared root surfaces in all deep gum pockets to stimulate the body’s own regenerative stem cells, reduce inflammation, inhibit growth of bacteria, aid in the reattachment of the gums, and promote osteogenesis (bone regeneration). A safe and effective anti-inflammatory medication is used temporarily to promote more rapid healing and stability of the gums by resetting the inflammatory response and boosting activation of regenerative cells (Periostat).
To understand more about the research and science behind this advanced protocol click here.
Watch this procedure on You Tube.
More cases: Perioscopy Case Studies, Before and After pictures, Advanced Cases.
RPE is completed in one appointment with local anesthetic, there is no need for repetitive visits as with other periodontal treatment modalities. There is no down time following RPE, making it very convenient for our many clients traveling in from out of state. Our clients do not need to alter their diet and they do not experience long term root sensitivity following RPE. Remarkable clinical results are achieved without surgery, including closure of deep gum pockets and bone regeneration. RPE is a definitive and affordable treatment option which can reduce or eliminate the need for periodontal surgery and extractions. View our testimonials
Before and after pictures and x-rays of actual RPE:












Above – Before RPE – 12mm pocket – advanced bone loss – this patient was advised by his periodontist he needed to have this tooth extracted and an implant placed. He chose RPE as a less invasive, more affordable option- see result below.


3 months after RPE – normal healthy tissue 3mm- bone fill well underway, no mobility, and no need for an extraction and implant. This tooth was treated in 2006 and is still healthy. This patient saved thousands of dollars in treatment costs by avoiding an extraction, bone graft, implant, and crown.










(This patient is a heavy smoker)












see before and after x-rays below












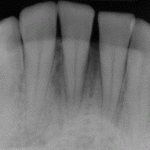
Before RPE – advanced bone loss #4
6 months after RPE – nice bone fill






The patient above was told she needed to have this tooth extracted and an implant and crown placed. She was also treatment planned for full mouth osseous periodontal surgery for multiple infections and deep pockets. Instead, she chose the option of RPE. She was able to avoid spending $12,000 for the full mouth surgery and the added expense of having an implant placed. Her total cost for full mouth RPE treatment was only $3000.


The above result has been maintained since 2006.


Before full mouth RPE -advanced case with generalized deep pockets – 3 years after RPE, complete health restored. More photos of this case below:






The patient above was told due to her hopeless advanced periodontal disease she would eventually lose all of her teeth. She was very embarrassed to smile due to shifting of the teeth from the advanced bone loss with deep pockets and was emotionally devastated before coming to PerioPeak. She now has tight healthy tissues with no mobility and no bleeding. This patient underwent orthodontic treatment after RPE to correct extrusions and malocclusion. She is elated with her results!


The patient above was facing the loss of her entire bridge due to advanced periodontal bone loss, 3 months after RPE she no longer had to worry. Health restored to the gums with nice bone fill on the x-ray.


The patient above was able to avoid extraction of the molar tooth, thus saving the bridge. She was able to avoid having an implant placed, followed by a new bridge for this area.




The case study below demonstrates well the speed at which healing occurs with RPE.













Before RPE – 11mm with heavy bleeding and a periodontal abscess clearly seen – 6 months after RPE 2mm very tight healthy tissue – see bone fill on x-rays below.



















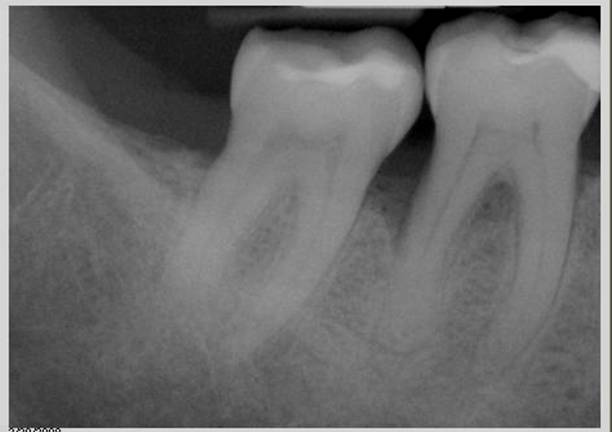


The above tooth was treatment planned for extraction by the periodontist. #31 presented with a 10mm distal defect, a 10mm furcation on the buccal, and mobility. Only 7 months after RPE, all periodontal probing depths are normal, there is no mobility, and the tissue is tight and healthy.
_____________________________________________
The RPE protocol is very specifically designed to arrest the chronic inflammation associated with periodontal disease, allowing long term healing and restoration of the gums to occur. RPE goes beyond the short term results seen with traditional non surgical treatment strategies – including the overuse of oral or locally applied antibiotics, and/or traditional laser periodontal therapy. View more case pictures.
One third of the population has a genetic tendency to develop periodontal disease, one half of those individuals will develop advanced periodontal disease, resulting in tooth loss. RPE can effectively interrupt and reverse this grim outcome for millions of individuals.
While no formal research yet exists on this three pronged innovative approach, there is impressive research on each technology studied independently, demonstrating efficacy in the treatment of periodontal disease. Pairing these technologies properly promotes “synergy” – the phenomenon in which the combined action of two or more things is greater than the sum of their effects individually. Because periodontal disease is multi-factorial, it can typically be more effectively treated using a synergistic approach.
Contact us for a complimentary consultation
For more information about sub-antimicrobial dose doxycycline 20mg go to host modulated therapy.
For more information about regenerative proteins (Emdogain) go to https://periopeak.com/bone-regeneration/